|
Click HERE to see full infogram
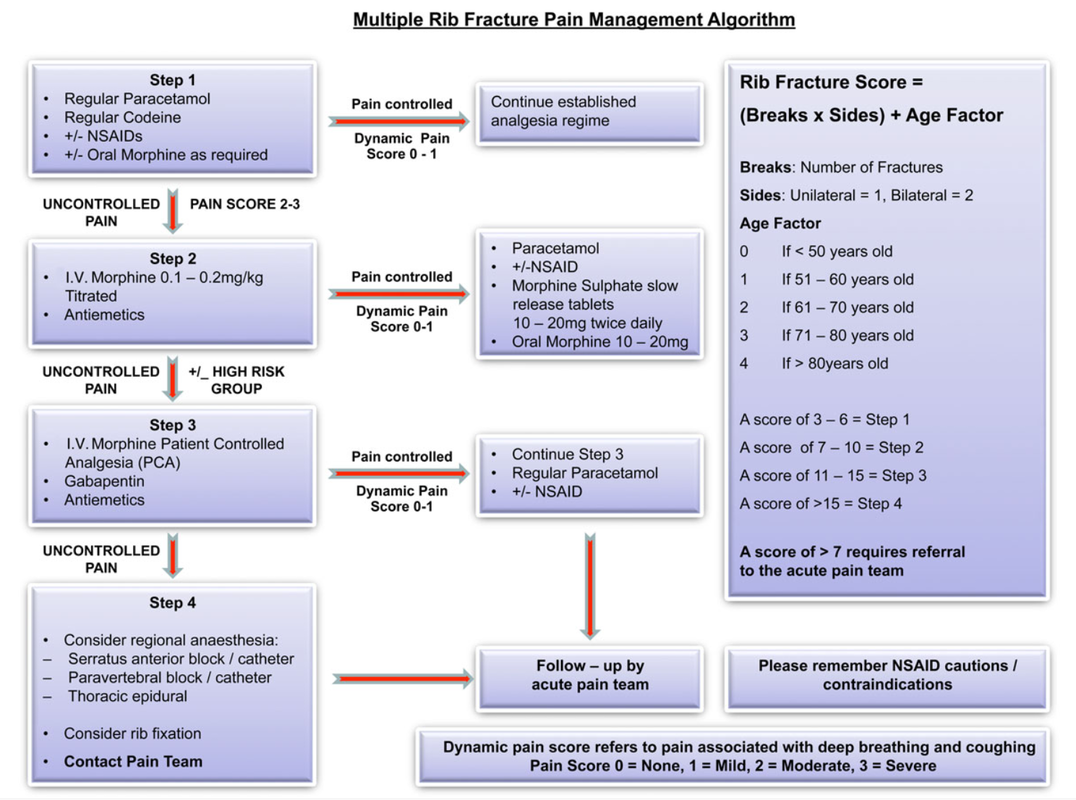
The above algorithm is taken from the BJA Education article, here.
NB: Regional techniques offer high levels of non-narcotising pain relief, such as intercostal blocks and s.anterior blocks +- catheters. (You will all know I am an advocate of the CERTA concept of pain relief, with non-opioids and RA techniques used whenever possible). With all the best will in the world, it is hard to find a trained individual to site or perform such regional techniques in an acute setting 24/7 and in a timely fashion, let alone have a service on the ward that is happy to look after different pumps/complications/troubleshooting etc. This is why this guide will focus on pharmacological management +- Thoracic Epidural where indicated/available. It is also worth noting that non-catheter blocks wear off at various rates depending on local analgesia used, so you still need to be aware of pharmacological management and the step-wise pain pathways. Should 24/7, quick-access Regional Anaesthesia be available in your hospital; this is a great asset and should be used in conjunction with your own local policies.
Rib fractures can be difficult to manage with respect to adequate pain relief and maximised chest safety. There is a high risk, in more complex fractures, of pneumothorax, haemopneumothorax, flail chest and great vessel injury. One of the most significant problems to prevent, (after PTX etc) is the acquisition of an atelectasis induced chest infection, particularly in those with concomitant chest disease and advancing age. You must be able to rapidly and safely control pain levels. We also know that a lot of patients can be managed on the ward with good nursing, physiotherapy and analgesia and that many are not admitted to ICU. It is worth noting that an HDU/ICU admission may be required if pain is not controlled and breathing becomes an issue - you should involve the pain and ICU teams early, but this should not substitute or preclude the admitting team & ED actively trying to control pain using the algorithm above. It will be useful to the acute pain teams to see which, if any, analgesia worked. All patients with rib fractures may not be admitted, but those who are sore enough to should have basic care (mentioned in the infograph) commenced IMMEDIATELY in A&E. Good regimes of escalating pain regimes must be in place from A&E and admission teams and NOT just wait for a pain team review, which can be after a busy weekend or the next working day. It may be nice to allow all patients to have a thoracic epidural sited, but this is not pragmatic in a busy NHS hospital; it will often be the next day or 'after the weekend'. They are also not required for every rib fracture patient. NEVERTHELESS, thoracic epidurals DO have benefit for those who have complex disease processes, fractures and advancing age. They probably should not be inserted due to inadequate attempts to control pain with more conventional pharmacological methods in most patient groups. Surgical wards are used to dealing with PCA's so they often become the first stop of acute pain management. Wards are often not set up to facilitate IV lignocaine/ketamine infusions; if your wards are - you should contact your local pain team to see whether these interventions might be utilised in your place of ward in lieu of a morphine PCA. Do not forget to write up emergency naloxone if using opioids alongside an anti-emetic regime. Here is the best BJA Education Article for scoring rib fractures with advice on pharmacy etc. A final note on pharmacy; PLEASE check the BNF for contraindications of medications in your patient. Renal function is also important with respect to opioids, NSAIDs and Gabapentin etc.
0 Comments
Leave a Reply. |
USE OF THIS WEBSITE IS SUBJECT TO AGREEING TO THIS DISCLAIMER
|
 RSS Feed
RSS Feed

Free to access Propofology Infograms, eBooks and selected YouTube videos by Dr. David Lyness are licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Please attribute all works: 'Based on a work by Dr. David Lyness' at www.propofology.com/resources.
|
Home
About Contact |
ALL SITE USERS SHOULD READ AND AGREE TO THE DISCLAIMER HERE.
Contact via Twitter |